
Why Your Client’s Gluteal Pain Isn’t Coming From the Glutes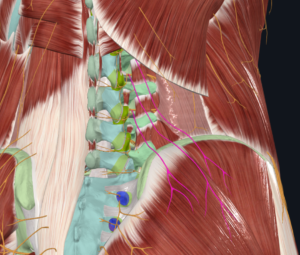
As manual therapists, we’ve all had the client who presents with persistent pain in the upper gluteal region — right over the gluteus medius and maximus. The instinct is to dig in, release the tissue, and work the area until it softens. But what if the pain isn’t originating there at all?
This is one of the foundational principles behind Physiokinetix Training: stop chasing the pain and start addressing a whole systems approach.
The Superior Cluneal Nerves: An Overlooked Source of Referred Pain
The superior cluneal nerves (also called the superior gluteal cutaneous nerves) are purely sensory branches arising from the lateral divisions of the posterior rami of spinal nerves L1–L3. They travel inferolaterally, crossing over the iliac crest, and provide sensory innervation to the skin of the lower back and upper buttocks.
Here’s the clinical problem: because these nerves originate from the lumbar spine and refer sensation to the gluteal region, pain felt in the buttock may actually be generated at L1–L3 — not in the gluteal muscles themselves. Research has demonstrated that lumbosacral nerve root irritation frequently produces referred pain to the buttock, posterior thigh, and calf in patterns that do not follow classic dermatomal maps. The buttock is the most common referral site across L3–S1 levels.
This means that when a client presents with upper gluteal pain, the source may be a nerve originating two or three spinal levels above — not the muscles under your hands. Spending excessive time massaging the gluteus medius and maximus may provide temporary relief through neurological modulation, but it does not address the underlying cause.
The Physiokinetix Approach: Thinking in Cross-Patterns, Not Segments
At Physiokinetix Training, we teach that the body does not function in isolated muscle segments. It operates through integrated myofascial sling systems that transmit force diagonally across the trunk during movement. One of the most well-studied of these is the posterior oblique sling: the latissimus dorsi connects through the thoracolumbar fascia to the contralateral gluteus maximus.
This is not theoretical. In vivo research has demonstrated that tensioning the latissimus dorsi produces measurable changes in passive hip properties on the contralateral side, confirming myofascial force transmission through the thoracolumbar fascia. Critically, this force transmission pathway is reduced in individuals with chronic low back pain — the contralateral connection weakens, and the system loses its ability to distribute load efficiently.
This has direct implications for our work. If a client presents with right-sided gluteal pain, the dysfunction may not be in the right gluteus maximus at all. It may involve:
- Reduced force transmission through the thoracolumbar fascia
- Weakness or inhibition of the left anterior oblique chain
- Poor neuromuscular coordination across the posterior oblique sling
In the Physiokinetix model, we address this by looking at the contralateral anterior chain — the opposite side’s obliques, adductors, and anterior hip musculature — to restore the balanced force couples that the body relies on during gait, rotation, and functional movement.
A Balanced Clinical Approach: The Physiokinetix Framework
Rather than spending the entire session releasing the painful gluteal muscles, Physiokinetix Training advocates for an integrated strategy:
- Understand the nerve anatomy. The superior cluneal nerves originate at L1–L3. Recognize that gluteal pain may be referred from the lumbar spine, not generated locally. This changes where you direct your assessment and treatment.
- Address the thoracolumbar fascia. This is the bridge between the upper and lower body — the highway through which the posterior oblique sling transmits force. Manual techniques directed at the fascial transition zone may be more productive than deep gluteal work.
- Strengthen the contralateral anterior chain. If the right gluteal region is symptomatic, evaluate and strengthen the left-sided anterior oblique sling — the internal oblique, external oblique, and adductors on the contralateral side. This restores balanced force couples across the pelvis.
- Integrate movement. This is the core of the Physiokinetix philosophy. Passive manual therapy alone has limited long-term benefit for low back and gluteal pain. Clinical practice guidelines consistently recommend active rehabilitation — strengthening, motor control, and functional movement — as the foundation of treatment. Manual therapy creates a window of opportunity. Movement fills it.
The Bottom Line
The superior cluneal nerves are a frequently overlooked source of gluteal pain. Understanding their anatomy — origin at L1–L3, course through the thoracolumbar fascia, and sensory distribution to the upper buttock — changes how we approach the symptomatic gluteal region. Combined with the cross-pattern sling mechanics at the heart of Physiokinetix Training, this knowledge moves us beyond “find the tight spot and release it” toward a whole systems approach to clinical practice.
The pain is in the glutes. The problem often isn’t.
Learn more at an upcoming workshop: templehp.com/workshops